Introduction
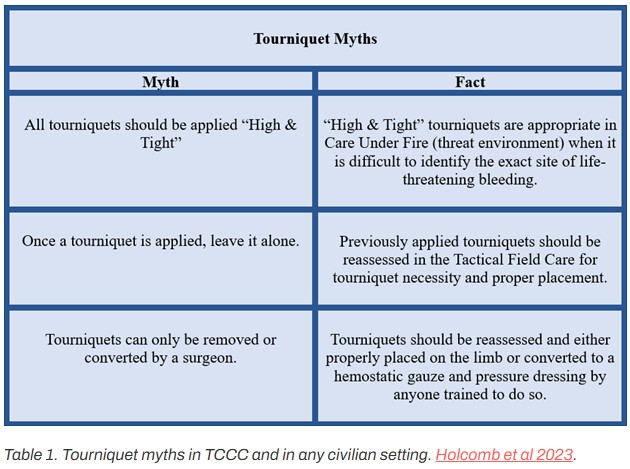
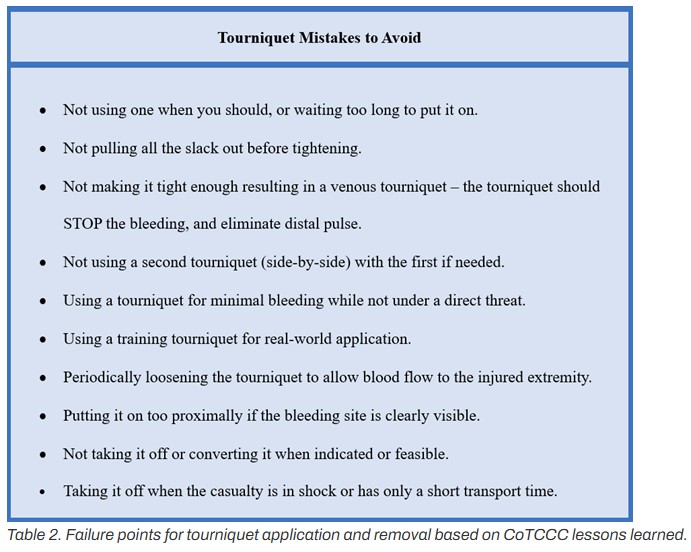
Prior to 2001, tourniquets (TQ) were inferiorly made, lacked evidence and effective training, and their use was discouraged. However, with effective modern TQ science, development, and TQ inclusion into the Tactical Combat Casualty Care (TCCC) guidelines, TQs became universally accepted by 2006 in the military as the primary option for extremity arterial bleeding. Eventually TQ use transitioned with success to civilian Emergency Medical Service/Fire Department personnel, Law Enforcement personnel, and first responders. Yet, there still is a need to overcome TQ myths (Table 1). Additionally, history reveals from WWII to present that mistakes will occur when applying a TQ (Table 2). For instance, many TQs have been applied to injured extremities without life-threatening bleeding in both military and civilian casualties. Many of these applied TQs were inappropriate since many were placed without visualizing the wound when not in a direct threat environment. In addition, when TQs are applied for over 2 hours, there will be progressive damage that may result in muscle necrosis, need for fasciotomy, renal failure, amputation, and death. This suggests a greater need for TQ education and training.
PDF: Tourniquet Lessons Learned from Ukraine and Israel
As an outcome from recent TQ lessons learned in the Ukraine and Israel wars, an article by Colonel John Holcomb, MD and colleagues was recently published in the Journal of Trauma, December 2023. They describe a renewed attention and education about how to avoid prolonged TQ application as recommended in the TCCC guidelines (See Massive Hemorrhage and Circulation sections – Table 3). It is our intent to provide the wilderness medical provider information about: 1) TQ replacement and TQ conversion (ideally performed no later than 2 hours after being applied); and 2) ensure the reader has up-to-date CoTCCC resources with the current TQ replacement/TQ conversion education and training.